‘CTCA has become a primary method for the diagnosis of Coronary Artery disease.’ (Journal of the American College of Cardiology, Aug. 2021)
Cardiovascular disease (CVD) is the leading cause of death worldwide. Early detection of significant Coronary Artery disease can enable early implementation of preventive or therapeutic measures.
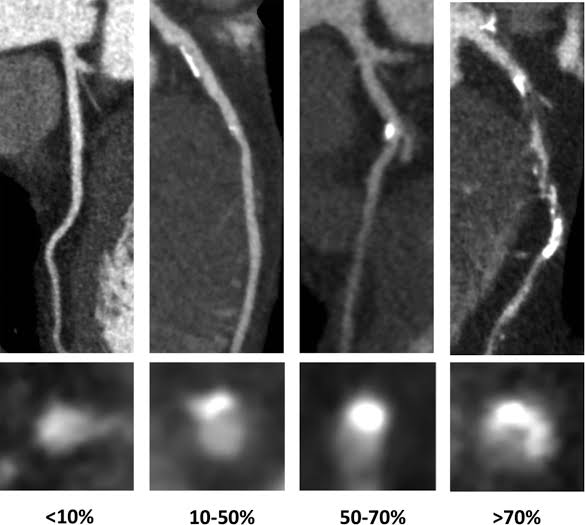
One of the primary methods for diagnosing Coronary Artery Disease (CAD) is CT Coronary Angiography (CTCA). CTCA is a rapid, non-invasive imaging method which accurately identifies the amount, extent, severity and composition of Coronary Artery plaque, and enables accurate assessment of the percentage of narrowing of affected vessels.
The high diagnostic accuracy of CTCA allows detection of significant coronary stenosis in patients without previously known Coronary Artery disease with a sensitivity of 95-99%.
Conversely, a normal CTCA study has a high negative predictive value of around 98%, effectively excluding significant Coronary Artery disease and avoiding the need for further imaging tests in patients with low to intermediate risk of CAD. (2)
Unlike CT Calcium Scoring, which simply measures the volume of calcified plaque in the wall of the Coronary Arteries to give an overall estimate of risk of Coronary Artery disease, CTCA directly demonstrates the both soft and calcified plaque, and accurately detects the presence and severity of Coronary Artery stenosis.
The ability to uniquely detect high-risk soft plaque is a fundamental advantage of CTCA over CT Calcium scoring. Unstable high risk fibro-fatty coronary plaques are typically non-calcified, and carry a higher risk of plaque rupture resulting in Major Adverse Coronary Events (MACE).
Acute coronary syndrome (ACS) most often arises from rupture or erosion of vulnerable soft plaques (4). Vulnerable or unstable coronary plaques are typically lipid-rich with a thin fibrous cap, or thin-cap fibroatheromas (4), and are not detectable with CT Calcium Scoring studies.
A 2018 article in Circulation : Cardiovascular Imaging, looking at clinical outcomes of patients with CTCA-detected coronary plaque found that 3.9% of patients with high risk soft plaque sustained Major Adverse Coronary Events (MACE) within 1.3 to 8.2 years, vs 1.2% for densely calcified, lower risk plaques.
New generation 640-slice CT scanners equipped with AI image enhancement enable ultra-low radiation doses for CTCA studies, dramatically reducing doses for CTCA compared to former generation scanners by up to 80%.
Coronary plaque composition is also an important prognostic determinant of CAD. CTCA is also accurate in coronary plaque characterisation, demonstrating key high risk plaque characteristics including positive remodelling, low attenuation lipid rich plaque (< 30 HU), a ‘napkin-ring sign’ and spotty calcification, all of which are associated with a higher risk of MACE. The large multi-centre ROMICAT-II study showed high-risk plaques on CTCA in patients with low to intermediate risk of CAD were associated with an increased likelihood of Acute Coronary Syndrome, independent of clinical risk factors.
Conclusion:
Ultra-low dose CT Coronary Angiography using current generation 640 slice CT scanners with AI enables fast, accurate and noninvasive detection of the presence, type and extent of Coronary atherosclerotic plaque, including identification of high risk soft plaque and measurement of coronary artery stenosis, using significantly reduced radiation doses, up to 80% lower than previous generation CT scanners.
Identification of mild coronary plaque allows implementation of lifestyle modification and preventative measures. The presence of more advanced obstructive plaque or significant coronary stenoses may warrant preventative or therapeutic medication, or consideration of interventional measures.
References:
1. Journal of the American College of Cardiology – ‘CT Coronary Angiography as a Primary Diagnostic Tool for Coronary Artery Disease’; Aug 2021
2. Sing Med J.; ‘Computed Tomography Coronary Angiography – Past, Present and Future‘; 2021
3. Circulation: Cardiovascular Imaging – ‘Vulnerable Plaque Detection by CT Angiography-Can We Improve Identification and Risk Stratification?‘; 2018
4. Circulation: Cardiovascular Imaging; ‘Computed Tomographic Coronary Angiography–Derived Plaque Characteristics Predict Major Adverse Cardiovascular Events- A Systematic Review and Meta-Analysis‘; 2018
5. Rev. Cardiovasc. Med.; ‘Identification and treatment of the vulnerable coronary plaque’; Veleen et al, 2022
6. BMJ – Heart; ‘Using radiation safely in cardiology: what imagers need to know‘; MC Williams et al; Feb 2019
7. Clinical Radiology; ‘The future of CT: deep learning reconstruction‘; McLeavy et al; 2021
**DLP = Dose Length Product (mGy.cm), an international standard measure of radiation exposure weighted for body region
I’m always happy to discuss individual cases with referring clinicians – if you’re a medical practitioner seeking an opinion on which imaging-guided pain management measures may be most appropriate and beneficial in an individual clinical situation, please feel free to contact me directly.
Dr Angus Watts
MBBS, FRANZCR
Diagnostic and Interventional Radiologist
Panorama Bulk Bills all Medicare-eligible studies including eligible CTCA referrals from any medical specialist.
Panorama also offers GP-referred CTCA studies at a heavily subsided fee of $350.