Lower back pain is one of the most common clinical presentations in general practice and emergency departments around the world, and around 80% of us will experience issues with back pain requiring management in our lifetimes.
Degenerative disc disease is so common with advancing age that from a radiological perspective it can almost be viewed as a normal part of the ageing process, and in many cases is asymptomatic in itself. Disc protrusions and degenerative osteophytes causing nerve root compression and radiculopathy, right through to spinal stenosis, are a common cause of morbidity in the acute and chronic setting.
From my own perspective, as a radiologist with subspecialty Fellowship training in both musculoskeletal imaging and interventional radiology, almost two decades of experience in the diagnosis and imaging guided management of back pain, working across two busy acute private hospitals and outpatient clinics, I’m often asked for an opinion on the likely pinpoint cause and imaging guided management options for patients with debilitating lumbar back pain, particularly in complex cases where scans demonstrate multiple potential sources of the patient’s primary symptoms.
As an interventional radiologist, I believe a critical part of successful imaging-guided pain management is to discuss and understand the patient’s specific symptoms, and correlate this with the imaging findings. In my experience, there is sometimes a disconnect between managing specific symptoms vs managing what is seen radiologically. Indeed, patients with complex back pathology may describe symptoms on the contralateral side or a different anatomical region altogether to the major imaging findings.
Our job is to understand the clinical and radiological picture as a whole, to optimise the accuracy of imaging guided pain management, and clinical outcomes.

Whilst the range of lumbar back pathology is vast, one of the commonest clinical decision-points for imaging guided management is differentiating facetogenic pain from radicular-type pain and spinal stenosis.
Plain films have a role as a screening tool in the assessment of a variety of lumbosacral pathology such as disc degeneration, assessing the presence and degree of spondylolisthesis, fractures, facet joint arthropathy and sacro-iliac joint pathology.
In the setting of radiculopathy or severe lumbago, CT and/or MRI have a key role in identifying and localising pathology such as disc protrusions, nerve root compression, facet joint pathology, synovial cysts and sequestrated disc fragments that may cause nerve root compression, and defining the presence and causes of spinal stenosis.
From a radiological perspective, I often ask patients some simple key questions that sometimes get lost amongst the deluge of clinical information that accompanies complex cases. What side is your pain on? Does the pain go down your leg? Not infrequently, this simple information, when combined with a review of the patient’s MRI or CT images, may prompt a review of the procedure and approach being considered.
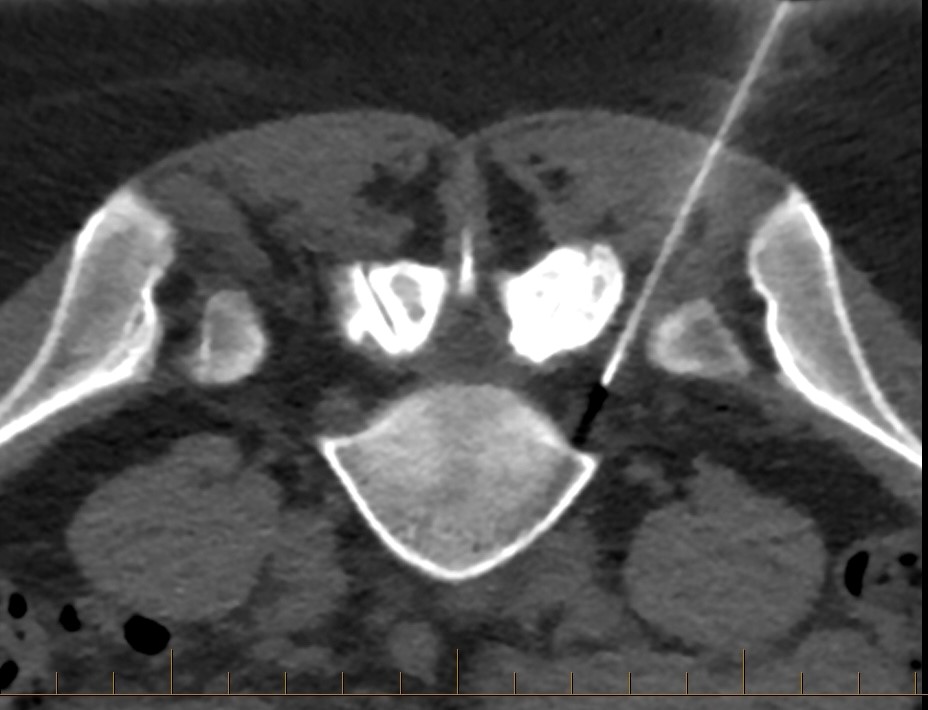
In some cases, particularly in the setting of multi-level facet joint arthropathy or multiple sites of nerve root compression, when a precise source of pain isn’t clearly apparent on initial imaging, a single targeted CT guided facet block (or nerve root sheath block) may be of diagnostic as well as therapeutic benefit, in localising the precise source of symptoms. If the symptoms persist, further targetted injections can be considered. This may sometimes be of additional diagnostic benefit compared to a broader approach of performing multiple injections in one sitting, although obviously in the setting of severe pain the blanket approach is likely to have better short term success.
Many spinal specialists refer patients with facetogenic pain for a targeted CT guided medial branch block to assist with pain localisation and diagnosis, prior to consideration of the longer-term analgesic measure of CT guided Radiofrequency medial branch nerve ablation, which offers many patients longer term relief from facetogenic pain in the setting of facet joint arthopathy and synovitis. We perform RF ablation radiologically under light sedation, with CT guidance allowing precise needle placement within a few mm, to optimise accuracy and efficacy.
CT guided epidural steroid injection is a common analgesic procedure we perform for a variety of clinical pictures, most commonly for patients with radiculopathy from spinal stenosis, large disc protrusions or multilevel degenerative nerve root compression. In straightforward cases of isolated nerve root compression, in general I often recommend trialling a CT guided nerve root sheath block if appropriate as an initial analgesic measure, then if symptoms persist stepping up to an epidural steroid injection if required.
I’m always happy to discuss individual cases with referring clinicians – if you’re a medical practitioner seeking an opinion on which imaging-guided pain management measures may be most appropriate and beneficial in an individual clinical situation, please feel free to contact me directly.
Dr Angus Watts
MBBS, FRANZCR