Shoulder pain requiring some form of management affects around a quarter of Australians in their lifetime, making it one of the most common and debilitating musculoskeletal complaints. The range of underlying pathology is vast, but from a primary care perspective, identifying or excluding some key treatable acute pathologies is an important first step in diagnosis and management.

From a radiological perspective, shoulder pathology can be categorised as –
Extra-articular conditions (eg – subacromial bursitis, rotator cuff pathology, subacromial impingement, os acromiale, AC joint pathology, biceps tendon pathology), and
Intra-articular conditions (eg – adhesive capsulitis, arthropathies, labral tears, SLAP tears, gleno-humeral instability, loose bodies etc)
A first line of investigation with plain X-Rays and Ultrasound is an excellent starting point for a variety of clinical presentations, including trauma, over-use injuries, impingement and frozen shoulder. The two modalities provide complementary diagnostic information, which can be broken down as –
X-Rays – fractures, glenohumeral dislocation/subluxation, AC joint pathology, calcific tendinitis/bursitis, arthropathies and calcific loose bodies, osseous pathology.
Ultrasound – rotator cuff pathology (tears, calcific and noncalcific tendinopathies), bursitis, biceps tendon pathology, impingement and AC joint pathology. Note these are largely extra-articular conditions.
MRI is the most sensitive and specific investigation for shoulder pathology, particularly in relation to the accurate detection and characterisation of rotator cuff pathology, intra-articular conditions such as labral and ligamentous tears, chondral injury and bone marrow pathology.
MRI Arthrography is the most accurate and sensitive imaging test for the investigation of gleno-humeral instability, the most common form being anterior instability (eg – recurrent dislocation in young adults). An MRI Arthrogram involves injection of MRI contrast dye (dilute gadolinium) into the gleno-humeral joint under CT guidance prior to MRI scanning. The study allows significantly better visualisation of the intra-articular structures including the labrum, biceps anchor, articular cartilage and capsule.
In my two decades of experience in interventional and musculoskeletal radiology, I’ve performed around 4000 MRI Arthrogram studies, and my patients overwhelmingly find it a quick procedure with minimal discomfort, which adds significant diagnostic information to the study.
CT generally has a complementary role to other modalities in a variety of settings such as the assessment of fractures, glenohumeral arthropathies, defining intra-articular loose bodies, and assessing glenoid morphology for pre-operative planning. CT is insensitive in the assessment of soft tissue pathology such as rotator cuff tears and bursitis.
Imaging Guided Management of Shoulder Pain
At Panorama Radiology Specialists, we offer the full spectrum of imaging guided pain management intervention for shoulder conditions, including intra-articular injections for AC and gleno-humeral arthritis, subacromial bursal and biceps tendon sheath injections, arthrograms, hydrodilatations, PRP injections and suprascapular nerve blocks.
Some common clinical examples include –
- Ultrasound guided subacromial bursal injection – typically used in the setting of bursitis, rotator cuff pathology and impingement. Using high resolution real time ultrasound, the needle tip is positioned with precision within the subacromial bursa (which is frequently just 2-3mm in thickness) followed by HCLA injection.
- Ultrasound guided biceps tendon sheath injection – real time precision placement of the needle tip within the biceps tendon sheath (with care to avoid the long head of biceps tendon fibres) followed by HCLA injection. The sheath is typically around 2mm in depth circumferentially around the biceps tendon.
- AC joint injection – needle tip placement within the capsular synovium of the AC joint and HCLA injection.
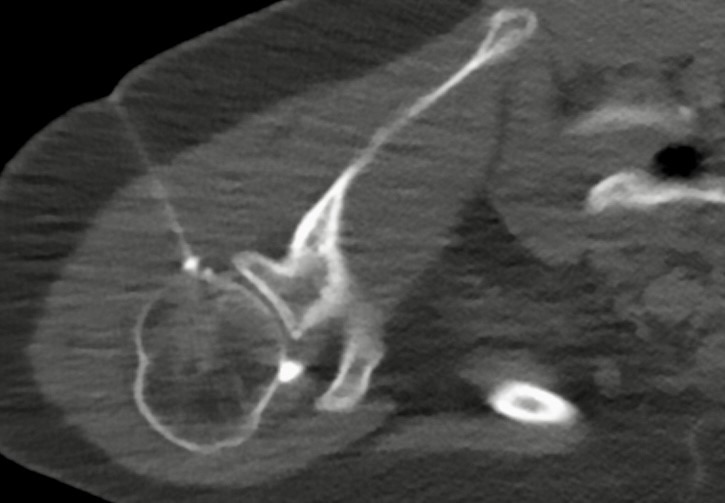
- CT guided glenohumeral joint injection – typically in the setting of arthropathies – precision CT guided intra-articular placement of the needle tip, with confirmation of intra-capsular positioning followed by HCLA injection.
- CT guided shoulder hydrodilatation – for adhesive capsulitis (frozen shoulder) – CT guided intra-articular needle placement confirmed, followed by injection of HCLA and saline to maximal capsular distension. Hydrodilatation may assist in improving the range of movement in adhesive capsulitis, by applying capsular tension and stretching, analogous to physiotherapy.
- CT guided suprascapular nerve block – may be beneficial in the setting of chronic shoulder pain (eg – arthopathies, frozen shoulder and rotator cuff pathology) – under CT guidance a needle tip is placed in the perineural tissues adjacent to the suprascapular nerve and HCLA injected. Patients with chronic shoulder pain may experience significantly reduced pain, improved sleep and range of movement.
I’m always happy to discuss individual cases with referring clinicians – if you’re a medical practitioner seeking an opinion on which imaging-guided pain management measures may be most appropriate and beneficial in an individual clinical situation, please feel free to contact me directly.
Dr Angus Watts
MBBS, FRANZCR